Improvement Achieved and a Dream Fulfilled
Improvement Achieved and a Dream Fulfilled
In 2008 the Director of Aged Care Services for the Rockhampton and Central West Health Services, Carmel Schweitzer took the rather bold step of joining the remote rural Multipurpose Health Services (MPHS) of the Queensland Health Service District into the QPS Aged Care Benchmarking program. The MPHS were all former acute care hospitals that have had their role transformed from predominantly an acute care role to one that is heavily focused on residential aged care, community care and some acute services e.g. small accident and emergency centres. Carmel realised, and explained to QPS, that the MPHS needed support to help managers and staff to focus more on their aged care role and to better understand the outcomes being achieved in aged care.
Carmel selected QPS Benchmarking to help for three reasons:
- QPS had been providing benchmarking services to the larger Rockhampton based dedicated aged care facilities since 2002.
- It was considered that the new QPS software platform could be easily managed by the onsite managers, even those with little IT experience or confidence in IT.
- The service model of a dedicated Principal Consultant could help facility managers to access support and guidance.
It would be fair to say, that in the beginning, not all of the MPHS managers considered that benchmarking could be applied in the MPHS setting. With the largest facility being just 20 beds some managers voiced the concern that they were "too small to benchmark". Some argued that the results would be skewed by the small number of residents. Others suggested that the local managers would not cope with the IT system.
Just 18 months down the track, it is refreshing to see comments such as those from Jennifer Williams at the Winton MPHS that read "it probably would be great for all of the sites (Queensland MPHS) to revisit the idea of this form of benchmarking just to identify gaps in service provision that primarily focus on the aged care component. The executives at the Winton MPHS already have decided that even if funding cannot be sourced in the service plan for 2010 - 2013 that the cost would be covered in the overall budget of the facility. This is because we see it being a great avenue for data collection that is neither cumbersome nor time consuming. Even for the techno illiterate like me." Editor: Jennifer may have judged herself harshly in the last sentence.
Improvements - A review of some MPHS selected KPI's
One of QPS Benchmarking's most popular KPI's is skin tears and this indicator is collected by all MPHS. The graph below shows the Management Report Trend Graph. This graph represents the collective data for all MPHS from December 2008 to March 2010.
It would be fair to say that although numerous MPHS scored above the average for skin tears there was suspicion from some managers that the above average results were due to the small number of residents in the individual facilities and that they may have just been unlucky during that first three months. When the second set of data came in and the overall skin tear rate increased a few of the MPHS managers took a second look and a couple of managers started drilling down into the incident data. Trends such as "most skin tears occurring during night shift from falling residents" were noted. At Baralaba, Helen Carbery delved further by reading all of the QPS Newsletter articles about skin tears and she summarised the strategies being applied elsewhere. A paper summarising the strategies used by other QPS Benchmarking clients was circulated to the other MPHS in the health service district. In other places, the managers found that by simply asking the question of staff about skin tear incidents and discussing the causes, that improvement began to be noticed. Overall the skin tear rate has dropped from approximately 80% to around the industry average of 30% over the past twelve months.
One of the most pleasing aspects of this improvement has been the sharing of information and strategies via the QPS Newsletter. One of the main reasons we benchmark is to search for best or better practice. By identifying the substantial opportunity for improvement and then trialling the strategies of others, the MPHS have demonstrated the benefits of benchmarking.
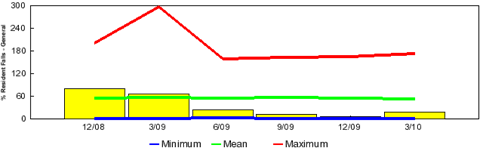
There has been a similar result for falls, one of the major problem incidents in aged care. Falls can result in skin tears and even more serious injury. The correlation between the falls and skin tears data is evident if you look at the two graphs together.
Example of Individual Facility Improvement
At the individual facility level we have seen some facilities show good signs of analysis at the time of data input and in some cases the small facilities have found it quite useful to use the QPS Data Input comment boxes as a way of recording all incidents and outcomes. At the Blackwater MPHS, the manager shows how she was able to link her results to a review of the incidents, actions taken and eventual outcomes. The comments on the graph below are from the Blackwater client comment boxes.
Summary
If benchmarking data is properly normalised and reviewed over time then it matters little whether you are big or small and it has been learned that intimate knowledge of the incidents can be a tremendous advantage once the outcomes or overall rates are better understood. When benchmarking commenced in the MPHS not all managers knew what a high skin tear or falls rate was.......they do now, and they act.
Postscript
Unfortunately Carmel Schweitzer died from cancer earlier this year. But if Carmel is able to somehow see Jennifer William's email or this article I am sure she would smile.
Article submitted by: Clinical Governance Unit, Central Queensland Health Service District
0 comments