Managing Medication Documentation Errors - with the help of other QPS Benchmarking Clients
Managing Medication Documentation Errors - with the help of other QPS Benchmarking Clients
Farr Home is a 16 bed high care facility in the central districts of Queensland. It is owned and operated by Queensland Health.Prior to becoming a member of QPS Benchmarking, the facility had been actively working on reducing the rate of medication errors through continual cycles of audit and education. Whilst the continual audits identified the problems, and education highlighted these issues to staff, sustained improvement proved difficult to achieve.
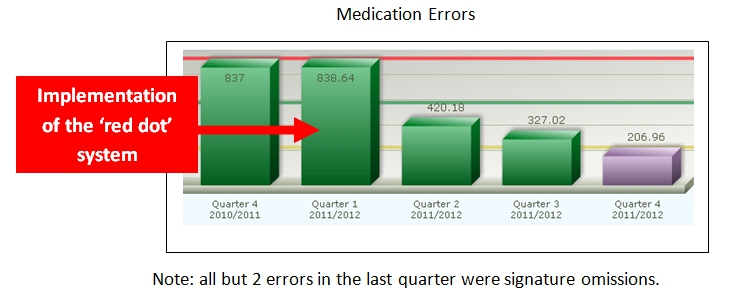
When Queensland Health joined QPS Benchmarking there was significant debate during the onsite education program about both the merits of benchmarking medication error rates and the systems used to collect data. As part of this discussion, the 'red dot' system used by The Whiddon Group's (TWG) Largs Lodge (QPS Newsletter, Volume 23 September 2006) was distributed and discussed. The article suggested one possible way to collect medication documentation errors and achieve improvement.
Following the QPS education, the facility Nurse Unit Manager returned to Farr Home and relayed to the rest of the staff the discussions held on the self-reported medication errors key performance indicator. The 'red dot' system first described by TWG Largs Lodge was considered at one of the regular monthly quality meetings and it was decided they give it a try.
"Whilst the continual audits identified the problems, and education highlighted these issues to staff, sustained improvement proved difficult to achieve."
For the past ten years Farr Home have had different medication times highlighted in different colours, this system was implemented following an increase in signature omissions. It has been effective but it has not achieved full compliance. It has however helped to make medication rounds easier for new staff and more streamlined.
To prevent interruptions during the medication round, it became the practice for the Nurse Unit Manager to take the cordless phone on a morning shift and staff members advised to approach medication administrators with only major concerns, thus allowing the Registered Nursing staff to give medications without interruption and to reduce the number of errors.
To establish an accurate base line, a more formal audit commenced detailing RN/EEN initials, resident, and time of each signature omission, to see if there was a particular trend. This was done using the 'red dot' system. The Nurse Unit Manager ensured each RN/EEN was sent the medication guidelines and expected responsibilities and accountabilities. All registered staff members were rostered to attend yearly medication competencies. As a final intervention, the Nurse Unit Manager commenced daily checks of medication charts at the completion of each day shift to ensure no signature omissions.

At first the checks have to be done on a daily basis, but over time and as the culture for self reporting has grown, the frequency of the checks has been gradually reduced and they are now done on a more random basis. Staff members from all shifts are now routinely highlighting errors as they see them. Night staff members, in particular, are often heard discussing errors with staff prior to the completion of their shifts, but the 'red dots' are still applied. From a data collection point of view they are also very easy to count.
Facility Manager Shelley Lee points out that the 'red dot' system may not be the solution for everyone. Shelley notes that she has been at the facility for 16 years and that many of her staff members have been there as long, if not longer. Staff turnover is very low and this "helps immensely to discuss and implement systems that are sustainable", says Shelley. At the time of writing this article Shelley also mentions that one of the Central Queensland University students remarked that of all the places she has trained in, Farr Home has the most stable and settled systems for resident management and documentation.
"Through benchmarking and the sharing of ideas we have now made both substantial and sustained improvement"
The low staff turnover also assists Farr Home to implement a very strong orientation program for clinical staff. Every new care staff member is assigned to the Aged Care Clinical Nurse to do all three shifts over a four day period. The key goal of this system is to get the new staff member orientated into the facility's systems and processes - and it works. This process has also helped embed the 'red dot' reporting process.
This may be a simple example but to Shelley Lee and her staff, it demonstrates one of the great benefits of benchmarking. "If during our education phase we had not shared the newsletter information about the 'red dot' system we may still be relying on the old system of audit and education, and very probably be struggling to achieve any real improvement. Through benchmarking and the sharing of ideas we have now made both substantial and sustained improvement." Shelley also claims that whilst large improvement has been achieved there is still room for further improvement.
It is noted, that like Farr Home, the facility that first described the 'red dot' system for recognising medication documentation errors (TWG Largs Lodge) was also a relatively small rural facility with low staff turnover and good systems for staff orientation.
0 comments