Optimising ACFI at TLC Aged Care Group
Optimising ACFI at TLC Aged Care Group
TLC Aged Care Group commonly known as the Tender Loving Care Aged Care Group is a family group that has been caring for the elderly since 1991. It has nine aged care facilities throughout Melbourne and Geelong.
TLC has been benchmarking its performance with QPS Benchmarking since January 2006. The organisation strives to provide modern aged care with a touch of old fashioned TLC. In order to provide such services financial resources are needed and as Lisa Papettas, the ACFI Manager for TLC explains, it is important that aged care facilities and managers optimise their opportunities through the ACFI system.
Through her work with the facility managers Lisa has been able to identify numerous opportunities for improvement and after being slightly behind the industry when ACFI first commenced TLC has in more recent times both met and exceeded industry trends.
As Executive Operations, Maree McCabe explains "benchmarking helped us to identify both the opportunity for improvement and to monitor the success of our strategies. Our work in this area helps us to maintain the TLC".
Overall Corporate Management Report TLC ACFI Behaviour Scores
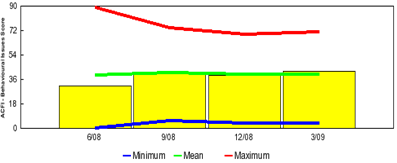
ACFI - A Paradigm Shift by Lisa Papettas, ACFI Manager TLC Aged Care
One can describe a paradigm as the set of practices that define a particular discipline. In our case, the "old paradigm" was RCS and the new is ACFI. Over the past 12 months we have moved from the old to the new.
The introduction of anything new (let alone something as all encompassing as a new funding model), brings with it a suitcase full of myths and half truths. This article endeavours to bust some of the most common myths and half-truths, whilst offering practical advice for ACFI practitioners. Providers need to revisit the claim process with this thought in the back of their minds:
"...are we claiming our funding entitlements and if not, what can we do to ensure we are?...".
If we do not claim our full entitlements then eventually it is the resident and aged care in general that misses out.
Whilst the industry's reaction and subsequent handling of the movement from RCS to ACFI post 20th March 2008 has been varied, many providers have found themselves struggling with the new set of disciplines. The range of industry experiences covers a broad spectrum. From negative financial impacts all the way through to significant rises in income and everything in between.
The funding pool hasn't changed but how we access it has. Therefore, as I write this article, the industry has within its ranks, a number of "winners and losers".
This is not to say that the "apparent" rises for some groups are necessarily a good thing. Whilst I'm a strong advocate for ACFI and its introduction, the ability of the model to place groups in a position of being in a "false sense of security" is dangerous and education on such matters must prevail. More on this later.
Why am I an advocate? As a clinician with over 25 years experience in the aged care sector, I believe in diagnosis driven care. That is, what we will be doing for our residents. Not what we are doing for them. This is subtle but at the heart of the issue. Until practitioners get their "heads around" this specific point, mistakes will be made. If you're reading this article right now, and you can't see the point, then STOP! You need to understand this BEFORE you proceed.
Managed correctly, residents and entities alike will win. More targeted funding is win-win, whether it's a "for-profit" or "not-for-profit" group or entity.
The ACFI philosophy has created a paradigm shift in how we claim for our funding. Under the previous RCS system we claimed based on what we were actually doing for residents. This was generally established through a series of assessment documents put out into the facility for the carers to complete and advise what care was necessary for a resident. Under ACFI we claim based on diagnosis driving the need for care, what care should be provided! This is the point where the provider can take the paradigm shift concept to a further extent and up skill the assessment process. The ACFI coordinator or clinician can review the diagnosis and discuss potential care needs with the care team. The carers should be considering the diagnosis before making a decision on what care should be provided. For example a resident with a history of falls may be quite independent in the areas of Activities of Daily Living. If however the resident was provided with assistance during these procedures the likelihood of falling would be significantly minimized. This is just one small example of the idea of diagnosis driving need for care.
From a funding perspective we have claimed our entitlement as supervision under ACFI 2-4 and from a care perspective the resident will be provided with the best and safest care outcomes.
There are many areas of ACFI that can be examined to not only drive better care outcomes but also ensure funding entitlements are appropriately claimed. In this discussion two such areas will be considered as an idea of how and why we need to develop better management strategies for ACFI assessment and claiming.
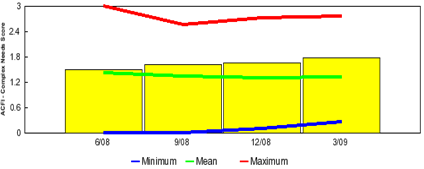
Pain management in the aged care setting is not only significantly under claimed in ACFI but could be considered to be undermanaged if ACFI claims are used as an indicator. According to the Department of Health and Ageing article Clinical Measures of Quality of Care and Quality of Life in Residential Aged Care Homes, March 2008, the prevalence of pain in residents in residential aged care facilities is as high as 70-80%. Pain management strategies such as heat packs, therapeutic massage and TENs machines not only provide positive management strategies but can also be claimed directly under ACFI 12 in three areas. If these strategies were to be introduced one would expect to see a significant increase in claim under ACFI 12. The ACFI Complex Needs benchmarking results show the progress being made at TLC.
Overall Corporate Management Report TLC ACFI Complex Needs Scores
There are many initiatives that can be implemented across organizations. One such example is the proactive approach TLC has made towards managing pain in their facilities. Pain management at TLC facilities has gone well beyond the administration of analgesia with many of the sites running regular pain management clinics for the residents.
The management of depression in the elderly person in the residential aged care setting has been further supported by the Department of Health and Ageing by the implementation of the compulsory assessment tool, the Cornell scale for depression assessment which is used under ACFI 10. Not only does the introduction of this assessment tool allow us to acknowledge depression in our elderly but also provides an accurate depiction of the degree of depression the resident is dealing with.
A recent interaction I had with a carer within a residential facility further highlighted the need for insistence of the use of this tool. During a review of an ACFI pack ready for submission I asked a nurse why she had not done a Cornell assessment on one of the residents. She stated that she has spent some time with the resident and she seemed fine to her. I explained to her that this is why we have the Cornell as a tool to assess depression because we as geriatric nurses do not have the expertise to identify the often subtle signs that depression often manifests in. A Cornell was subsequently completed on the resident resulting in a medium score of 18. A score of 18 using the Cornell depression scale would indicate moderate interference with a person's ability to function and participate in regular activities.
In a report to the Australian Government Department of Health and Ageing, the Hammond Care Group described the results of the Challenge Depression Project examining the management of depression in residents of aged care homes in Australia (2004c). The findings were that 51 per cent of high care and 30 per cent of low care residents who were able to complete the Geriatric Depression Scale were depressed; and 38 per cent of high care and 26 per cent of low care residents who were able to complete the Cornell Rating Scale (for the severely cognitively impaired) were depressed. The figures alone place a strong emphasis on the need to introduce compulsory completion of Cornell assessments within the residential setting to not only make sure a resident's depressive state is assessed but to also ensure funding entitlements are being claimed.
TLC's success in obtaining funding entitlements using ACFI can be attributed to the provision of significant resources that have been directed toward the management of ACFI.
Furthermore, TLC has developed a holistic approach to people, processes and skills that ensures ongoing education and communication regarding ACFI. This we feel guarantees better care and revenue outcomes. Win-Win and a bit more TLC!!
0 comments